Clinical and Radiation Oncologists based in Pretoria and Kempton Park in Gauteng, South Africa
Author: Dr Bassa Oncology
Dr Bassa oncology are oncologists based in Pretoria and Kempton Park, Gauteng. The practice focuses on Radiation therapy, Chemotherapy as well as palliative care.
Just as your period ends (or at the same time each month if you do not have periods) check for any change in the normal look and feel of your breasts. Report any changes to your doctor or nurse. Go for regular breast exams and ask about a mammogram.
Step 1: Lying Down
Lie down on your back with a pillow under your right shoulder.
Use the pads of the three middle fingers on your left hand to check your right breast.
Press using light, medium and firm pressure in a circle without lifting your fingers off the skin.
Follow an up and down pattern.
Feel for changes in your breast, above and below the collarbone and in your armpit.
Repeat on your left breast using your right hand.
These steps may be repeated while bathing or showering using soapy hands.
Step 2: In front of a mirror
Look for changes from normal, Inspect your breasts in four steps
Hold arms at your side
Hold arms over your head
Press your hands on your hips and tighten your chest muscles
Bend forward with your hands on your hips
WARNING SIGNS
See your doctor if you notice any of these in your breasts:-
Lump, hard knot or thickening
Swelling, warmth, redness, or darkening
Change in size or shape
Dimpling or puckering of skin
Itchy, scaly sore or rash on the nipple
Pulling in of your nipples or other parts
Nipple discharge that starts suddenly
New pain in one spot that does not go away
Dr Leiyah Bassa recommends the following: –
Monthly breast self-examination starting by the age of 20.
Clinical breast examination by a trained medical professional at least every 3 years starting at the age 20, and annually after 40.
Annual screening mammography for woman starting at the age 40.
For more information give us a call on 011 975 5655
A seven-year-old boy has become the first person in the country to receive volumetric arc therapy to treat his leukaemia.
The therapy was performed on the boy recently at Netcare Unitas Hospital in Centurion.
“The total body irradiation treatment was done in order to destroy the cancer cells in the young boy’s blood ahead of a bone-marrow transplant that he was scheduled to undergo just days after the completion of the radiation therapy,” said Dr Sheynaz Bassa, a clinical and radiation oncologist at the hospital.
“As far as we are aware, this is the first time in SA that a leukaemia patient has been treated using volumetric arc therapy prior to bone marrow transplantation,” Bassa said.
According to Bassa, a combination of radiotherapy, which uses high energy X-rays, and chemotherapy, which uses drugs given intravenously to kill cancer cells, is traditionally used to irradiate the entire body to destroy cancer cells in leukaemia patients before their bone marrow transplantation.
“Using traditional techniques, full-body irradiation is usually a long and laborious process involving complicated manual planning techniques, with the patient sitting in an uncomfortable treatment position for a long period of time.
“It also often requires production and use of cumbersome lead blocks to shield important organs like the lungs which are radiosensitive. The accuracy in the radiation dose to these organs is reduced due to the manual planning techniques and the patient does not have the benefit of a CT [computed tomography] scan being used in the planning,” said Bassa.
“Newer, more advanced technologies such as volumetric arc therapy allow for simpler, rapid and more effective full-body irradiation treatment delivery. This therapy is quicker, easier and provides us with information regarding the organs we are trying to protect, making it considerably safer. Lead blocks are no longer required, as the volumetric arc technology has built in capability to shape fields around the organs as the therapy is delivered.”
According to Bassa, in the boy’s case the radiation therapy planners did extensive research before deciding on the use of volumetric arc technology, drawing on international experience in which a similar treatment approach had been used for leukaemia to ensure the most accurate planning and treatment possible.
In an attempt to slow the speed of the spread of the COVID-19 the following measures have been implemented at Dr Bassa Oncology.
Measures put in place for the rooms:
Any patients exhibiting flu like symptoms will be prohibited from entering the practice (sore throat, coughing, running nose etc)
D germ sanitizer will be available on the arrival at the rooms, please ensure you sanitize your hands when you arrive and leave the practice.
No more than 1 family member is to accompany the patient.
Only the patient will be allowed in the chemo room.
No children will be allowed in the chemo room.
Please arrive at your appointment on time, if you do arrive early and will need to wait more than 10 minutes, we may request for you to wait in your car and will phone you as to when you can come to the rooms.
No patient that has been in contact with travellers from aboard, or travelled abroad within the last few weeks will be allowed in the rooms.
The practice has reverted back to normal business hours – Mon-Fri 8:00-16:00 for treatments.
Please contact the practice on 0119755655 for an appointment or any further assistance
Please inform us if you have:
Travelled abroad in the last two weeks.
Been in contact with anyone who has travelled abroad.
Have any symptoms of COVID-19 (Flu like Symptoms)
Been in contact with anyone that presents symptoms of the disease or anyone proven to have the contracted the disease.
The following symptoms are common for COVID-19:
Fever.
Coughing.
Shortness of breath or difficulty breathing.
Please assist the medical community and by practising the following hygiene measures:
Wash your hands often with soap and water for up to 20 seconds or use an alcohol-based hand sanitizer.
Cover your mouth and nose with your elbow or a tissue when you cough or sneeze. Dispose of the tissue once used and try not make use of a handkerchief.
Avoid touching your face, ie eyes, nose and mouth if your hands aren’t clean.
Avoid close contact with anyone who is sick.
Avoid sharing dishes, glasses, bedding and other household items if you’re sick.
Clean and disinfect surfaces you often touch ESPECIALLY MOBILE DEVICES. Please leave cellphones at home where at all possible.
Stay home from work and avoid public areas if you’re sick.
If you are experiencing any symptoms of COVID 19 please Whatsapp on +27600123456 or contact the hotline on 0800 029 999
Diarrhea is one potential side effect of cancer treatment. Radiation therapy to the abdominal area (mid-section of the body) can cause diarrhea, as can certain chemotherapy medications. If you struggle with diarrhea, there are several things you can do to address the problem and help your body
The most important thing you can do to control diarrhea during cancer treatment is to take medications as prescribed. As with many treatment side effects, prevention is more effective than cure. Once diarrhea is very severe, it can be more challenging to bring under control.
Severe diarrhea causes dehydration and lose of important electrolytes (minerals), including sodium and potassium. This can be a life-threatening situation, so do not ignore diarrhea. If your medical team prescribes medication to prevent diarrhea, do not wait until you have diarrhea to take it. For some cancer treatments, taking anti-diarrheal medications before the problem occurs is part of the plan.
Diarrhea Diet: Using Food To Better Manage Diarrhea
In addition to medical management, the following tips and tricks will help you manage diarrhea:
Eat more high-soluble fiber foods including plain oatmeal, white rice, ripe bananas, applesauce, white toast, canned fruit without the skins, such as peaches and pears, white pasta noodles, cream of rice cereal, and plain unsweetened crackers.
Drink 8 cups of non-caffeinated fluid each day to prevent dehydration. Try water; coconut water; decaf, chamomile, and ginger teas; ginger ale; rice milk; and diluted fruit juices and nectars, such as peach, pear, mango, or papaya nectar (avoid grape and prune juices).
Avoid Milk and milk products. Exceptions are buttermilk and yogurt, which are often tolerated because lactose is altered by the presence of Lactobacillus. Processed cheese may also be tolerated because the lactose is removed with the whey when it is separated from the cheese curd. Milkshake supplements such as Ensure are lactose free and may be used.
AVOID THE FOLLOWING
Whole-bran bread and cereal.
Nuts, seeds, and coconuts.
Fried, greasy, or fatty foods.
Fresh and dried fruit and some fruit juices such as prune juice.
Raw vegetables.
Rich pastries.
Popcorn, potato chips, and pretzels.
Strong spices and herbs.
Chocolate, coffee, tea, and soft drinks with caffeine.
Alcohol and tobacco.
FOODS TO EAT
Fish, poultry, and meat that is cooked, broiled, or roasted.
Bananas, applesauce, peeled apples, and apple and grape juices.
White bread and toast.
Macaroni and noodles.
Baked, boiled, or mashed potatoes.
Cooked vegetables that are mild, such as asparagus tips, green and waxed beans, carrots, spinach, and squash.
Mild processed cheese, eggs, smooth peanut butter, buttermilk, and yogurt.
Helpful hints
Ingest food at room temperature.
Drink 3 LITRES of fluid per day. Allow carbonated beverages to lose carbonation before being ingested.
Add nutmeg to food, which will help decrease mobility of GI tract.
Start a low-residue diet on day 1 of radiation therapy treatment.
MEDICATIONS THAT MAY BE PRESCRIBED
1 Lomitil, Gastron,Immodium
2 Kantrexel,Smecta, Pectin
3 Buscopan, Colofac
4 Codeine Phosphate, Morphine
Rehydrate with a rehydration solution, Energade, Isotonic Game etc
When should you call your doctor?
Diarrhea typically causes stomach cramps and loose, watery stools. Mostly it’s an inconvenience. But if your symptoms persist or get worse, it could be a sign of something more serious. Diarrhea can also lead to other problems, such as severe dehydration.
Some signs and symptoms are more serious than others are. Call your doctor right away if you have any of the following:
Six or more loose bowel movements a day for more than two days
Blood in your stool
Inability to urinate for 12 hours or more
Inability to drink liquids
Weight loss due to diarrhea
Diarrhea after several days of constipation
Severe abdominal pain
Fever of 101 F (38.3 C) or higher
Shaking chills
If your diarrhea doesn’t seem severe but starts to interfere with your daily activities, such as if you’re concerned about leaving home or going somewhere without a bathroom nearby, talk to your doctor. If abdominal cramping is keeping you from your daily activities, discuss this with your doctor, as well.
Skin changes are common and expected during radiation therapy. Each person reacts to treatment in a different way. The likelihood and severity of a skin reaction depends on:
The area being treated
The type and dose of radiation given
Whether or not you are also getting chemotherapy
After 2 or 3 weeks of radiation therapy, your skin may become pink or tanned. As your treatment continues, your skin may become bright red or very dark. Your skin may also feel dry and itchy and look flaky. Some people develop a rash or blisters in the treatment area. These blisters may open and peel. If you develop skin reactions, it will most likely improve 3 to 4 weeks after your treatment is finished.
Caring for Your Skin During Radiation Therapy
Keep your skin clean
Bathe or shower daily using warm water and a mild, unscented soap. Examples of soaps you can use include Neutrogena®, Dove®, and Cetaphil®. Rinse your skin well and pat it dry with a soft towel. When washing, be gentle with your skin in the area being treated. Do not use a washcloth or a scrubbing cloth or brush. The tattoo marks you received before treatment are permanent and won’t wash off. You may get other markings during treatment such as an outline of your treatment area with a purple felt-tipped marker. You can remove these markings with mineral oil when your radiation oncologist says it’s okay.
Do not use alcohol or alcohol pads on the skin in the area being treated.
Moisturize your skin often
If you are likely to get a skin reaction, your nurse will recommend that you start using a moisturizer. You should start using it the first day of your treatment to minimize the reaction. If you are not likely to develop a skin reaction, you will not need a moisturizer unless your skin becomes dry or itchy. The best moisturizer is bland, non fragranted aqueous cream. If the itching is severe then a mild steroid may be prescribed.
Apply the moisturizer at least 2 times a day.
If your radiation treatment is in the morning, apply it:
After your treatment
Before you go to bed
If your radiation treatment is in the afternoon, apply it:
In the morning before your treatment
Before you go to bed
On days you are not being treated, apply it:
In the morning
Before you go to bed
Do not wash off the moisturizer before your treatment. Your skin could become irritated.
Avoid irritating your skin in the treatment area
Wear loose-fitting, cotton clothing over the treated area.
Use only the moisturizers, creams, or lotions that are recommended by your doctor or nurse.
Do not use any of the following in the area being treated:
Makeup
Perfumes
Powders
Aftershave
Do not shave the treated skin. If you must shave, use only an electric razor.
Do not put any tape on the treated skin.
Do not let your treated skin come into contact with extreme hot or cold temperatures. This includes hot tubs, water bottles, heating pads, and ice packs.
Do not apply any patches to the treated area, including pain patches.
If your skin is itchy, do not scratch it. Ask your nurse for recommendation on how to relieve the itching.
If you have no skin reactions, you can swim in a chlorinated pool. However, be sure to rinse off the chlorine right after getting out of the pool.
Avoid tanning or burning your skin during and after you are finished with treatment. If you are going to be in the sun, use a PABA-free sunblock with an SPF of 30 or higher. Also, wear loose-fitting clothing that covers you as much as possible.
If you have any silver-containing bandages, remove them and clean the area before treatment.
We are fortunate (despite gripes from smokers themselves) in SA to have legislature which restricts public exposure to cigarette smoke. This may be inconvenient to smokers but by making it difficult and inaccessible (taxes), the habit is less common. For those who are skeptical regards the risk of cancer and smoking, the following article from http://www.cancerresearchuk.org/cancer-info/healthyliving will be interesting reading.
Thanks to years of research, the links between smoking and cancer are now very clear. Smoking is by far the most important preventable cause of cancer in the world. Smoking accounts for one in four UK cancer deaths, and nearly a fifth of all cancer cases.
In the UK, smoking kills five times more people than road accidents, overdoses, murder, suicide and HIV all put together.
Which cancers are caused by smoking?
Smoking causes more than four in five cases of lung cancer. Lung cancer has one of the lowest survival rates of all cancers, and is the most common cause of cancer death in the UK. The good news is that most of these deaths are preventable, by giving up smoking in time.
Smoking also increases the risk of over a dozen other cancers including cancers of the mouth, larynx (voice box), pharynx (upper throat), nose and sinuses, oesophagus (food pipe), liver, pancreas, stomach, kidney, bladder, cervix and bowel, as well as one type of ovarian cancer and some types of leukaemia. There is also some evidence that smoking could increase the risk of breast cancer.
Not all smokers get cancer. Why?
You may know someone who smoked all their lives but lived to a ripe old age. Or you may know someone who never smoked but got cancer anyway. Does this mean that smoking doesn’t really cause cancer?
Not at all. Years of research have proven that smoking causes cancer. But this doesn’t mean that all smokers will definitely get cancer or that all non-smokers won’t. It means that smoking greatly increases the risk of this disease. Smokers are, on average, much more likely to get cancer than non-smokers.
In a similar way, we can say that eating sugary foods is a cause of tooth decay. This doesn’t mean that all children who eat sugary foods will end up with decayed teeth. It means that, on average, children who eat lots of sugary foods are more likely to develop tooth decay than those who avoid such foods.
The fact is that half of all smokers eventually die from cancer, or other smoking-related illnesses. And a quarter of smokers die in middle age, between 35 and 69.
Our How do we know? page has more information on the evidence linking smoking to cancer.
How does smoking cause cancer?
Tobacco smoke contains more than 70 different cancer-causing substances. When you inhale smoke, these chemicals enter your lungs and spread around the rest of your body.
Scientists have shown that these chemicals can damage DNA and change important genes. This causes cancer by making your cells grow and multiply out of control.
Giving up makes a difference
Thanks to research, health campaigns and new policies, the number of smokers in the UK has halved in the last 50 years. Because of this, the number of people who die from lung cancer has also halved. Clearly, giving up smoking saves lives.
But there is still a long way to go. Lung cancer is still the second most common type of cancer in the UK and kills over 35,000 people every year. And there are signs that the number of people who are quitting is starting to match the number who are taking it up.
If you are a smoker, giving up smoking is the best present you can give yourself. There are many techniques you can try to help you join the increasing numbers of smokers who are quitting for good. You can find more advice on quitting in this section.
What is radiation therapy? When is it used?
Radiation therapy uses high-energy particles or waves, such as x-rays, gamma rays, electron beams, or protons, to destroy or damage cancer cells. Other names for radiation therapy are radiotherapy, irradiation, or x-ray therapy.
Radiation therapy is one of the most common treatments for cancer. It’s often part of the treatment for certain types of cancer, such as cancers of the head and neck, bladder, lung, and Hodgkin disease. Many other cancers are also treated with radiation therapy.
Radiation can be given alone or used with other treatments, such as surgery or chemotherapy. In fact, certain drugs are known to be radiosensitizers (ray-dee-oh-SENS-it-tie-zers). This means they can actually make the cancer cells more sensitive to radiation, which helps the radiation to better kill cancer cells.
There are also different ways to give radiation. Sometimes a patient gets more than one type of radiation treatment for the same cancer.
How does radiation therapy work?
Radiation therapy uses special equipment to send high doses of radiation to the cancer cells.
Most cells in the body grow and divide to form new cells. But cancer cells grow and divide faster than many of the normal cells around them. Radiation works by making small breaks in the DNA inside cells. These breaks keep cancer cells from growing and dividing, and often cause them to die. Nearby normal cells can also be affected by radiation, but most recover and go back to working the way they should.
Unlike chemotherapy, which exposes the whole body to cancer-fighting drugs, radiation therapy is usually a local treatment. It’s aimed at and affects only the part of the body being treated. The goal of radiation treatment is to damage cancer cells, with as little harm as possible to nearby healthy tissue.
Some treatments use radioactive substances that are given in a vein or by mouth. In this case, the radiation does travel throughout the body. But for the most part, the radioactive substance collects in the area of the tumor, so there’s little effect on the rest of the body.
WHAT IS A PORT A CATH
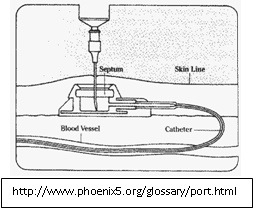
Port-A-Cath is an implanted venous access device, also known as an implanted port, placed completely under the skin. It is used for patients who require frequent or continuous chemotherapy administration.
The Port consists of three parts:
-The portal: a small chamber sealed with a septum on the top, made of silicone
-The catheter: a thin flexible tube
-The catheter connector: connects the catheter to the portal
Why is a Port-A-Cath used in chemotherapy?
The catheter of the port sits inside a large central vein. The port is used to collect blood samples and to give chemo medications. Before using, the skin over the port is cleaned and then a special needle is used to puncture the septum of the port, which is connected to the catheter. This allows for collection of blood samples as well as direct administration of medication into the bloodstream, using the port. After every infusion/injection, the port is flushed with heparin solution or once every 4 weeks if the port is not used regularly.
How is the Port-A-Cath used?
Generally chemotherapy drugs are very toxic and irritating to the skin, tissues and veins. Giving such potent medications into a small vein can irritate and cause inflammation of these blood vessels, resulting in long-term scarring and blockage of these veins. Also, giving chemo into a small vein allows the medication to leak into the nearby tissues and cause tissue damage. As a result, such medications are administered into a large central vein so that they can be immediately diluted by a large volume of blood and be delivered effectively throughout the entire body. The chemotherapy drugs are usually administered into the Internal Juglar or Subclavian vein; but sometimes Brachial vein may also be used. Studies show that the use of the Port-A-Cath in treatment & management of cancer patients, results in shorter hospital stay, less nursing time spent trying to access veins, preservation of the small veins, fewer emergency visits, decreased cost of therapy and overall greater patient satisfaction. As a result, the port serves a safe and effective route of giving chemotherapy drugs.
How is the Port placed?
Placing the Port is a small surgical procedure and takes less than an hour. It is performed by surgeon in theatre. The procedure involves a 3cm skin incision on the chest wall for the port pocket and 5mm incision in lower neck to enter the vein. The port is placed completely inside the body. One end of the catheter is inserted into the vein while the other end is connected to the portal, under the skin. The tip of the catheter lies in a vein just above the heart.
Port placement:
Chest-placed system: The Port is placed in the chest and the catheter is inserted into a vein in the chest. The tip of the catheter lies in a vein just above the
Generally, the patients can go home two hours after the procedure or after the effect of sedation has worn off. However, patients are advised to not drive or operate any machinery for 24 hours. When the incisions are healed, one can notice a small bump under the skin.
What preparations are required for the port implantation?
One is asked to not eat or drink anything starting at midnight before the procedure day. Clear fluids and medications are allowed till the time of procedure but it is best to verify with your doctor. Also mention to your doctor if you are on aspirin, plavix or warfarin to find out when to discontinue these medications prior to surgery. The medications can be resumed the day after the procedure. If you are sick with an active/ongoing infection, your doctor might choose to postpone your Port placement.
What are the aftercare precautions required?
-Keeping the port-site clean at all times is very crucial. If an access needle is in place, it is covered with a dressing to keep the site clean and prevents the needle from dislocating. If there is no needle in place, one can bathe/shower regularly.
-After surgery, it is normal to have some redness and tenderness at the area of incision which should resolve in 24-48hrs. However if you continue to have redness, tenderness, swelling or drainage from the site for more than 2-3 days or notice any other unusual skin changes, contact your doctor immediately.
-Avoid any strenuous activities involving the chest/arms for at least ten days. If the port is not used in 7 days after placement, follow-up with your doctor for a wound check and dressing change.
-If your portacath is no longer being used, you need to follow-up with your doctor every 4 weeks and get it flushed with saline water and locked with heparinized saline to prevent formation of blood clots.
-Minimize physical activities that involve excessive, repetitive upper extremity motion: such as swimming, golfing, weight-lifting as there is risk of catheter damage/ fragmentation (breaking). Check with your doctor to make sure you take proper precautions while engaging in such activities.
What are the potential problems /risks associated with Port-A-Cath?
-Risk of infection: although the risk of infection with the port is minimal, catheter-related bloodstream infection is a concern in cancer patients. This can be prevented by keeping the port site clean, using antimicrobial catheters and antibacterial solutions to flush the catheter. If infected, the port is removed and one is treated with appropriate antibiotic medications.
-Risk of forming clots: After months of insertion, clots can form in the catheter. This is prevented by flushing the catheter regularly after blood draws and not giving any contrast through the port. Patients do not need to be on any treatment to prevent clot formation in the Port-A-Cath.
-Air outside the lungs: at the time of port placement air can leak out of the lungs but usually resolves with time.
-Irritation or blistering of skin where chemotherapy is being given
-Catheter dislocation if not properly secured with sterile tapes or surgical strips
-With the use of modern imaging technology, there is very little risk of bruising, bleeding or damage to the blood vessels.
How long does the Port-A-Cath need to stay in place?
The port can stay as long as your doctor wants. Talk to your doctor or nurse about how long your port needs to stay in place.
Is it ok to have MRI with the Port in place?
Port-a-cath is MRI conditional, which means that they may safely undergo magnetic resonance imaging with magnetic field strength of 3.0 or lower. However do mention that you have a port-a-cath placed prior to having an MRI done.
Will it be ok to go through security alarms/metal detectors with a port?
Metal detectors will not harm the Port-A-Cath. The Port will not activate the security alarms. However since the sensitivity of metal detectors varies, it might be helpful to have your Port Identification Card with you.
Additional guidelines for your Port.
-Do not inject any fluids or solutions in your port unless you have been asked to do so by your doctor or nurse.
-Inform your doctor if you notice that fluids are not flowing freely through the port and stop any infusion at that time.
-Inform your doctor if you notice any skin changes, such as redness, swelling, or drainage at the site of Port placement.












You must be logged in to post a comment.